ADRENAL SURGERY
Minimally Invasive Adrenal Surgery in Melbourne
Dr Saam Tourani is a Melbourne-based specialist endocrine surgeon with dedicated expertise in adrenal surgery. Adrenal tumours — including hormone-producing and non-functioning lesions — require careful multidisciplinary assessment before surgery is considered. When indicated, most adrenal operations can be performed using minimally invasive endoscopic retroperitoneal technique, allowing faster recovery and excellent outcomes in experienced hands. Dr Tourani works closely with endocrinologists and radiologists to ensure accurate diagnosis, thorough hormonal evaluation, and precise surgical planning tailored to each patient.
Understanding the Adrenal Glands
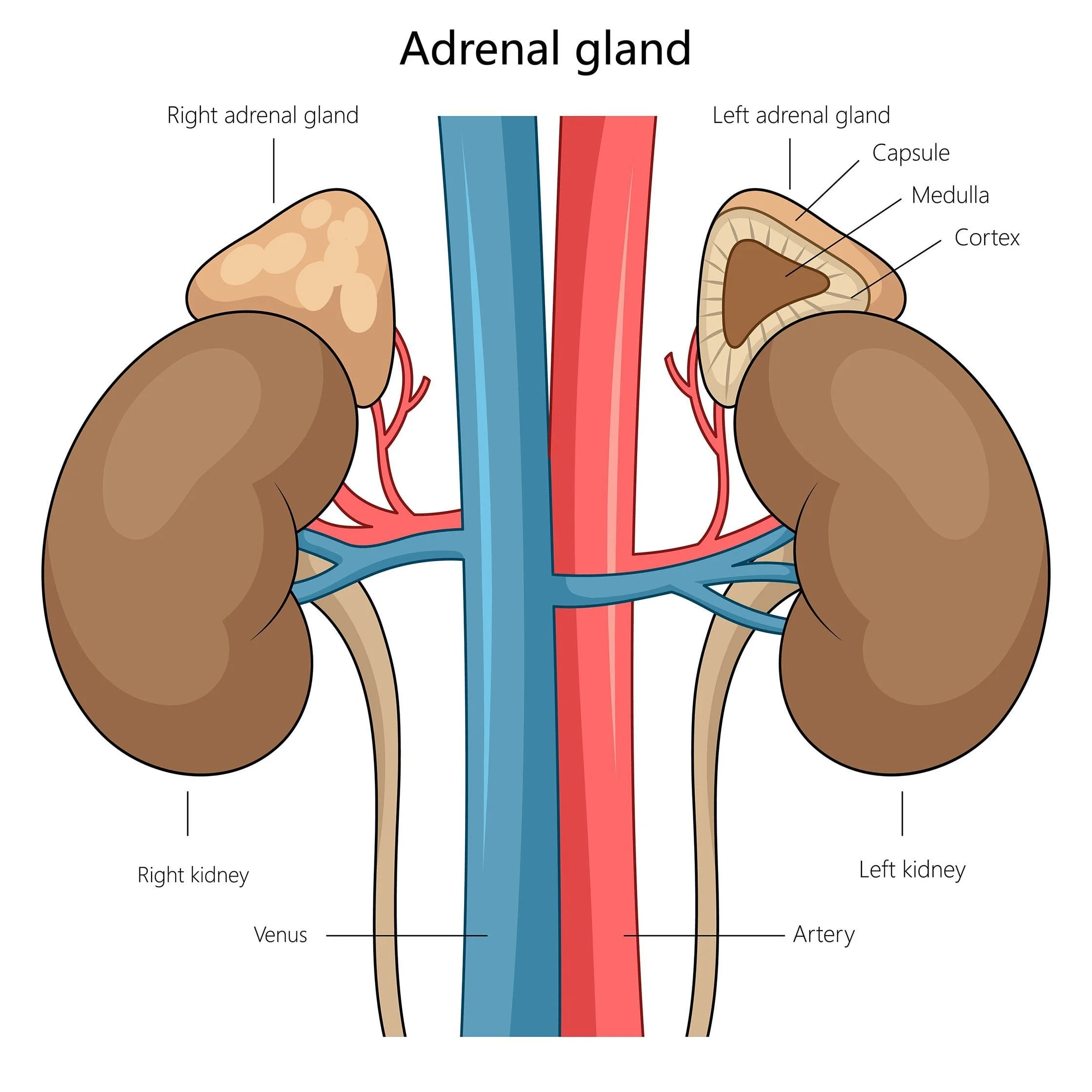
The adrenal glands are two small, triangular-shaped organs located above each kidney. Though small in size, they are powerful endocrine organs responsible for producing essential hormones such as:
Cortisol – the body’s stress hormone
Aldosterone – regulates blood pressure and salt balance
Adrenaline and noradrenaline – help respond to stress
Sex hormones – such as androgens (in small amounts)
Surgical Adrenal Conditions

Adrenal Adenoma
A benign tumour of the adrenal gland. Most are non-functioning and discovered incidentally on scans (so-called "incidentalomas"), but some produce excess hormones and require treatment.
Pheochromocytoma
A rare tumour that produces excess adrenaline, causing episodes of high blood pressure, headaches, palpitations, sweating, and anxiety. Untreated, it can be dangerous.
Cushing’s Syndrome
Is caused by an adrenal tumour producing too much cortisol. Patients may experience weight gain (especially in the face and abdomen), thinning skin, easy bruising, fatigue, and high blood sugar.
Conn’s Syndrome (Primary Hyperaldosteronism)
Is caused by an overproduction of aldosterone, leading to high blood pressure and low potassium levels. Surgery is often curative for unilateral cases.
Adrenal Cancer
A rare and aggressive tumour requiring urgent surgical removal, often with additional treatments depending on the stage and spread.
Diagnosis and Assessment
Diagnosing adrenal conditions — particularly those involving hormone overproduction — requires a high degree of diligence, experience, and attention to detail. Many adrenal disorders, such as Cushing’s syndrome, primary aldosteronism, or pheochromocytoma, present with subtle and non-specific symptoms. These changes often develop insidiously over months or years, and are frequently mistaken for common lifestyle-related issues such as high blood pressure, weight gain, fatigue, or anxiety.
Because of this, adrenal hyperfunction is often underdiagnosed or misattributed to other causes. I take great pride in conducting a comprehensive and systematic assessment, starting with a thorough history and physical examination, followed by targeted biochemical testing, hormonal profiles, and high-resolution imaging.
Every case is reviewed meticulously — I go through each result with a fine-tooth comb to ensure that no detail is overlooked and that any diagnosis is both accurate and meaningful. My goal is not just to name the condition, but to identify those patients who will truly benefit from surgery with real, long-lasting improvements in their health and quality of life.
In appropriate cases, surgical removal of the adrenal gland (adrenalectomy) can lead to significant and often curative changes — such as resolution of hypertension, correction of hormonal imbalances, or prevention of serious complications.
When is Adrenal Surgery Needed?
Surgery is generally recommended when:
The adrenal tumour is producing excess hormones
The adrenal adenoma is larger than 4–5 cm (higher risk of cancer)
There is radiological concern for malignancy
The tumour is producing local pressure symptoms
For a detailed discussion of surgical approaches to adrenal conditions — including the state-of-the-art retroperitoneal endoscopic adrenalectomy — please refer to our dedicated blog on this topic.

Blog: Adrenal Gland Surgery
Why Choose a Specialist Endocrine Surgeon?
Adrenal surgery is technically demanding and requires a detailed understanding of complex hormonal physiology and retroperitoneal anatomy. The adrenal glands sit close to major blood vessels, including the inferior vena cava and renal vessels, making precision and experience essential for safe surgery.
A specialist endocrine surgeon is trained not only in operative technique, but also in the careful interpretation of biochemical testing and imaging required to diagnose adrenal hormone disorders accurately. Proper patient selection is critical — not all adrenal tumours require surgery.
Dr Saam Tourani combines meticulous hormonal assessment, multidisciplinary collaboration with endocrinologists and radiologists, and advanced minimally invasive techniques to deliver safe, evidence-based adrenal surgery tailored to each patient.
Frequently Asked Questions
-
When performed by an experienced endocrine surgeon, adrenal surgery is generally safe. The adrenal glands sit close to major blood vessels, so specialist expertise and careful planning are essential to minimise risk.
-
Recovery largely depends on the surgical approach. Following minimally invasive retroperitoneal approach most patients are discharged the following day and back to normal activities within a few days.
-
This depends on the underlying condition and whether one or both adrenal glands are removed. Many patients require no long-term medication after removal of a single adrenal gland, but some may need temporary or permanent hormone replacement.
-
No. Many adrenal tumours are benign and non-functioning. Surgery is typically recommended when the tumour produces excess hormones, is large, or has concerning imaging features.