BREAST RECONSTRUCTION IN MELBOURNE
Your Journey, Your Choice
Breast reconstruction involves a range of surgical techniques used to restore the shape and appearance of the breast following mastectomy or extensive breast surgery. Reconstruction can be performed at the time of cancer surgery or as a delayed procedure, using implants, autologous tissue (such as DIEP flap), or a combination of approaches. Dr Saam Tourani offers expert breast reconstruction in Melbourne, combining oncological priorities with aesthetic principles to deliver a personalised approach that optimises both natural outcomes and long-term wellbeing.
Classification of Breast Reconstruction

Breast reconstruction aims to rebuild the breast following mastectomy. If you are advised to have a mastectomy for breast cancer, breast reconstruction can improve your body image and self-esteem, helping the process of recovery on a physical, emotional and psychological level. Breast reconstruction is now an integral component of breast cancer therapy and any woman undergoing mastectomy should have the opportunity to discuss her reconstructive options with her surgeon before the procedure, both in the public and the private sector.
Breast reconstruction can be classified based on the composition as well as the timing relative to mastectomy, as summarised in the table below.
| CLASSIFICATION OF BREAST RECONSTRUCTION | |
|---|---|
| Composition | |
| Autologous (tissue/flap) | e.g., LD, DIEP, or TUG flap |
| Prosthetic (implant) | subpectoral or prepectoral, one-stage or two-stage |
| Combined | flap reconstruction + a small implant for added projection |
| Timing | |
| Immediate | at the time of mastectomy |
| Delayed | reconstruction of flat chest wall following total mastectomy |
| Delayed immediate | insertion of tissue expander at the time of mastectomy followed by tissue reconstruction down the track (usually following radiotherapy) |
Implant or Tissue Breast Reconstruction?
Breast reconstruction may be done either with your own tissue that is relocated as a flap from another part of your body onto your chest (autologous reconstruction) or with the use of silicone implants (prosthetic reconstruction). Although falling out of favour, a combination of tissue and implant reconstruction may also be used as well when there is not enough tissue to achieve the desired projection with a full autologous reconstruction. However, in most of these cases addition of fat grafting can provide the extra volume required therefore avoiding using a prosthetic material all together.
Implant reconstruction is by far the most common type of breast reconstruction performed worldwide. This is due to multiple factors:
Lack of suitable donor sites for tissue reconstruction
Extra costs and skillsets required for tissue reconstruction
Additional scars and complications associated with tissue reconstruction

The implant technology has significantly improved over the years, and we now have a wide range of safe silicone implants available to suit most patients’ anatomies and desires. Our improved understanding of the surgical oncology of the breast has allowed less invasive mastectomies with preservation of skin, nipple, underlying pectoral muscle and ligamentous boundaries of the breast which will serve as a perfect template to fill in a with suitable silicone implant avoiding the added operative time, complexity, and complications of tissue reconstruction. In addition, the availability of a wide range of synthetic meshes and allografts and fat grafting has significantly added to our armamentarium for a durable, appealing and safe implant reconstruction.
Having said that, autologous reconstruction offers some unique advantages over prosthetic reconstruction and if available should be offered to patients undergoing mastectomy.
Advantages of Tissue Reconstruction
Long-term durability: Although breast implants don’t have an expiry date, the average shelf-life for breast implants is 15 years and more than 60% of women will need some sort of revision surgery within this time for rupture, capsular contracture or other complications. On the other hand, tissue reconstruction is rather a one-time, long-term investment. Your initial extra operating and recovery time is well spent for years of natural look and feel.
Avoid foreign materials: Infection is the biggest risk associated with the use of any foreign body material and occurs in about 10% of implant reconstructions. In addition, other risks associated with the use of breast implants include implant rupture, rotation, migration, rippling, capsular contracture and Implant Associated Anaplastic Large Cell Lymphoma (BIA-ALCL).
More natural feel and appearance: Despite the advancement in implant technology and reconstruction techniques, still tissue reconstruction offers the most natural look and feel to the reconstructed breast. In addition, it is more congruent with the rest of the body as it goes through aging and weight fluctuations. This can be particularly important for women who desire a more organic look and feel. However, some women may prefer the augmented breast look that is offered by implants.
Better symmetry: Tissue reconstruction may allow for a more symmetrical outcome, particularly when combined with procedures like fat grafting or breast reduction of the unaffected side to match the reconstructed breast. Matching an implant reconstruction with the contralateral breast is particularly challenging and often needs a smaller implant placed in the unaffected side to achieve symmetry.
Improved outcome with radiotherapy: Implant reconstruction and radiotherapy don’t go well together. This is due to increase skin shrinkage and capsular contracture associated with radiotherapy. Although implant reconstruction is not contraindicated, tissue reconstruction is the preferred form of reconstruction if post-mastectomy radiotherapy is planned.
Immediate or Delayed Breast Reconstruction?
Clearly from an aesthetic and psychosocial point of view, immediate reconstruction is preferred. By undergoing immediate reconstruction your surgeon will be able to preserve skin and the anatomical landmarks of your breast which will allow for a better aesthetic outcome, and you don’t have to go through the emotions of waking up from the general anaesthetics with a flat chest. However, in certain situations you may prefer a delayed reconstruction. There is often a lot to be considered and discussed if you are having breast reconstruction which you may find overwhelming. In particularly advanced cases delayed reconstruction may allow for a quicker progression through surgery and adjuvant therapy with less potential for delay.
Delayed immediate reconstruction is an alternative approach often employed in the setting of post-mastectomy radiotherapy. As mentioned before, implant reconstruction and radiotherapy don’t go well together. However instead of doing an immediate tissue reconstruction and then radiating the new reconstructed breast, in delayed immediate reconstruction a tissue expander is placed to preserve the skin and the anatomical landmarks in the first stage. The adjuvant therapies including radiation are then delivered, followed by second stage autologous reconstruction. With this approach the potential damaging effect of radiation on the reconstructed breast is avoided. In addition, a complex lengthy tissue reconstruction is reserved for a more convenient time following delivery of more urgent adjuvant therapies. Moreover, the patient may feel less pressured with many decision makings required in relation to both cancer therapy and breast reconstruction.

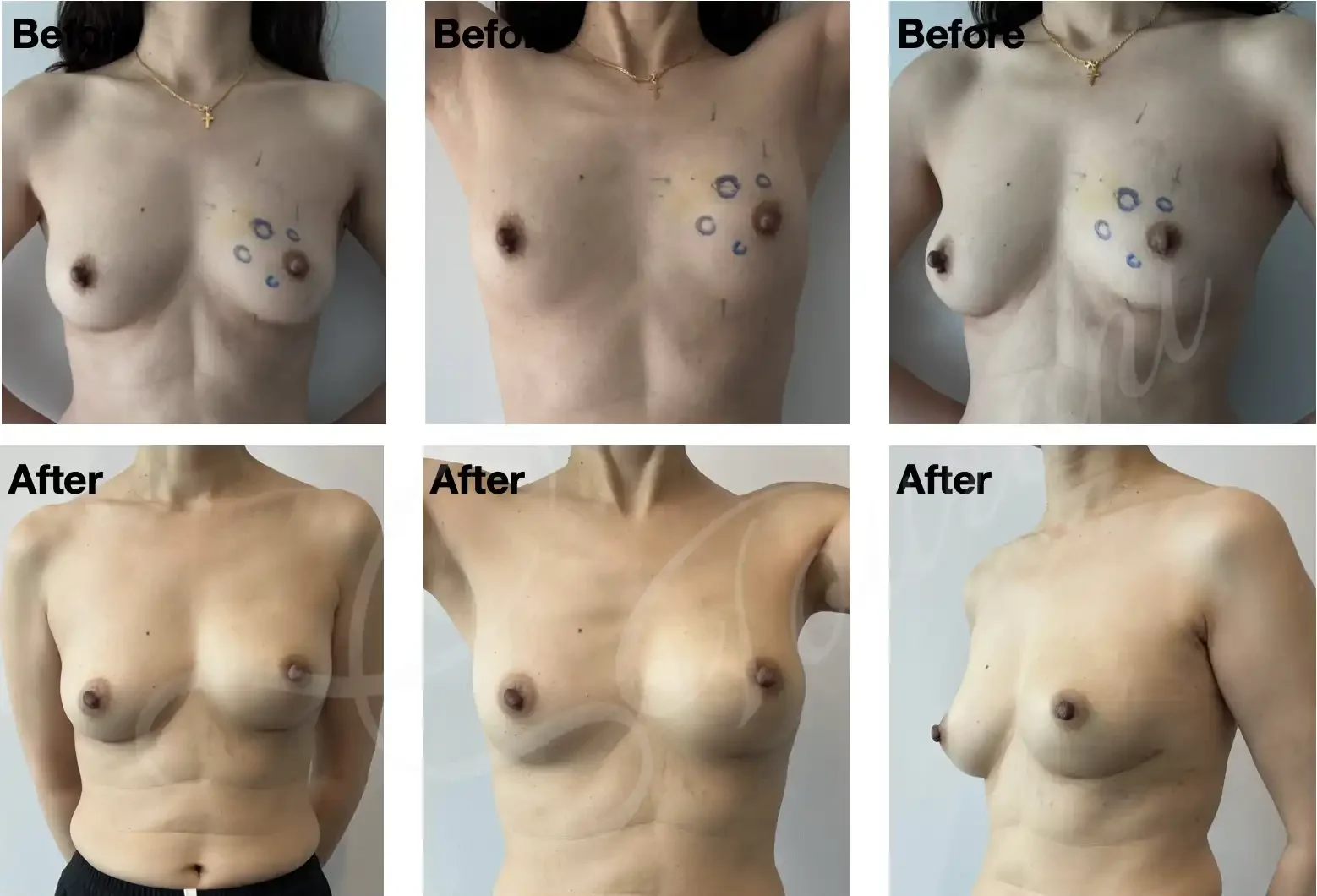
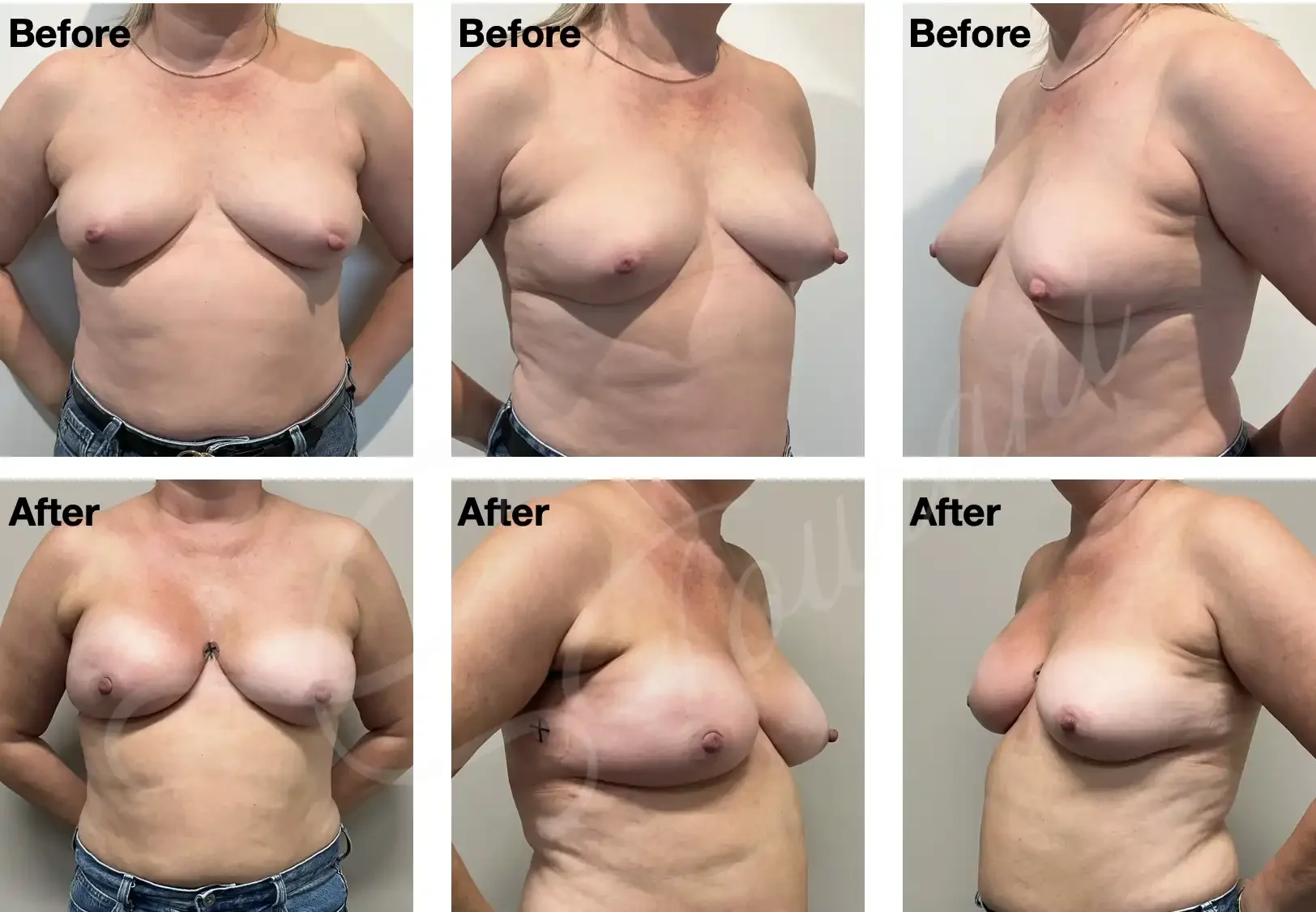
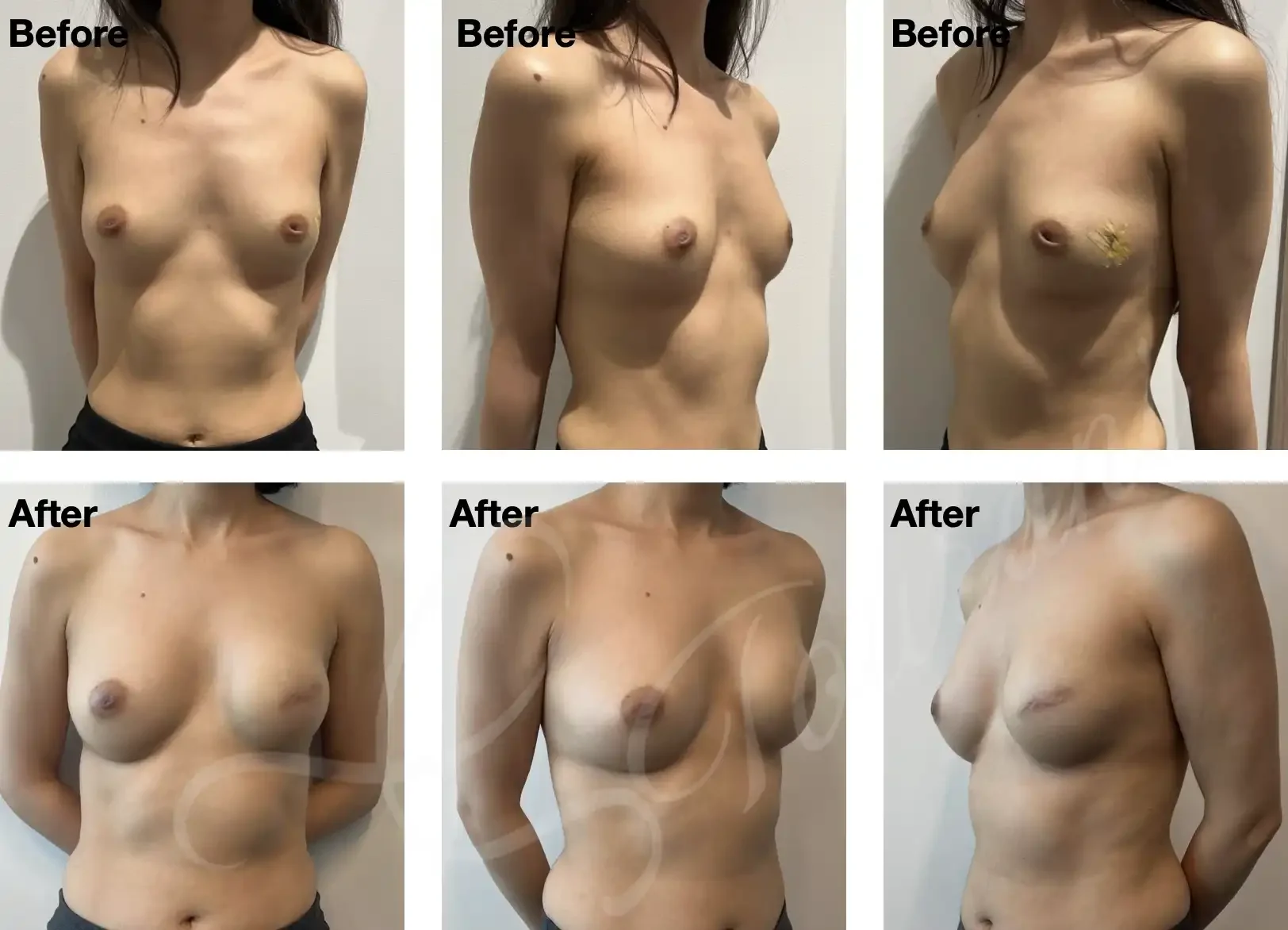
Breast Reconstruction – Before & After Gallery by Dr Saam Tourani

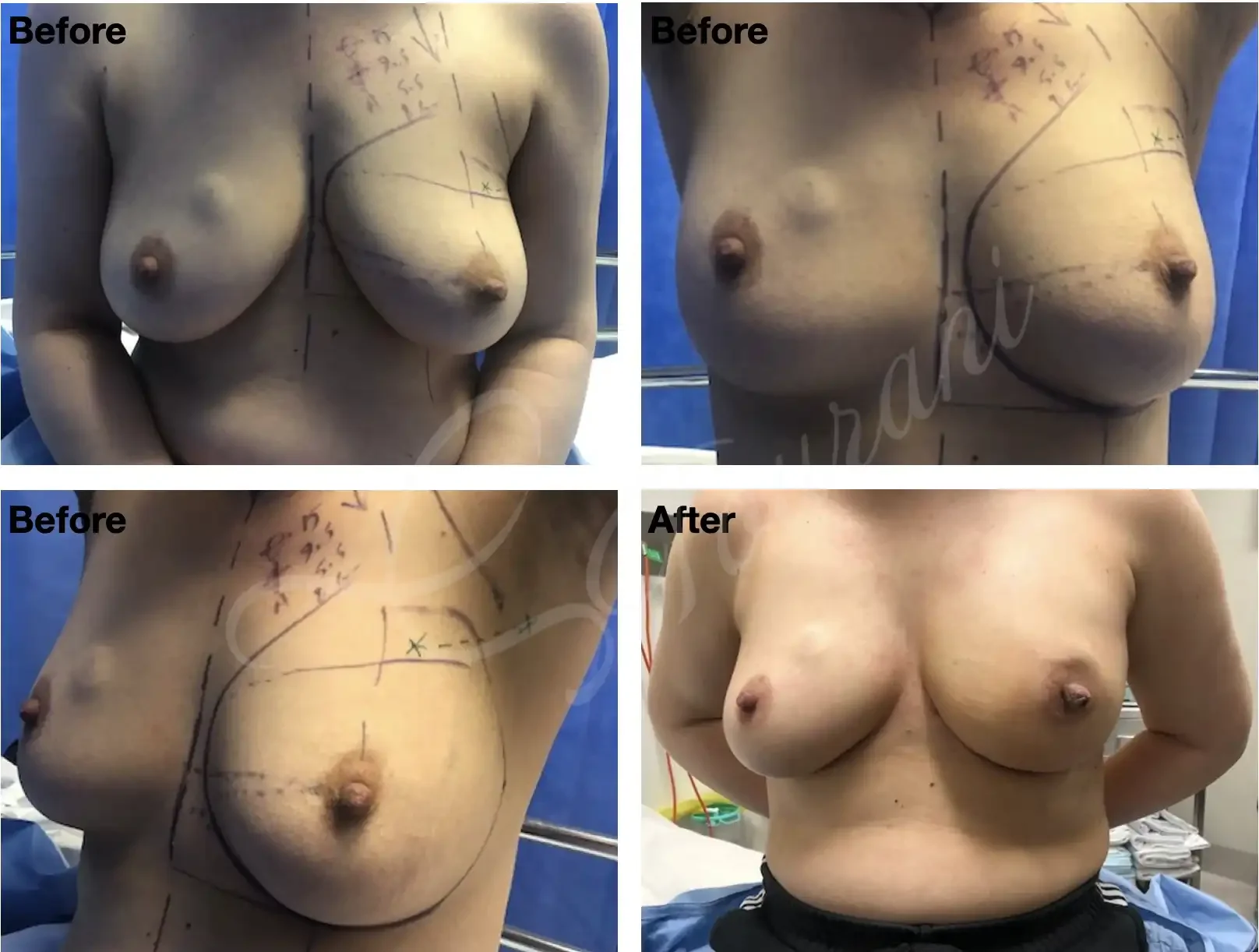
Case #301: Right skin reducing mastectomy and delayed immediate reconstruction with autologous LD flap. Images are 1 year following adjuvant radiotherapy. Awaiting right nipple reconstruction/areolar tattoo and left symmetrising breast reduction.
Case #302: Left nipple sparing mastectomy and immediate delayed reconstruction with autologous LD flap. Images are 1 year following adjuvant radiotherapy.

Case #303: Left skin reducing mastectomy + immediate autologous LD flap reconstruction following neoadjuvant chemo and radiotherapy for an inflammatory breast cancer. Images are two weeks following surgery.

Case #304: One year post right skin reducing mastectomy + immediate Autologous LD flap reconstruction. Optional second stage will involve right nipple reconstruction/areolar tattoo and symmetrising left breast lift/reduction.
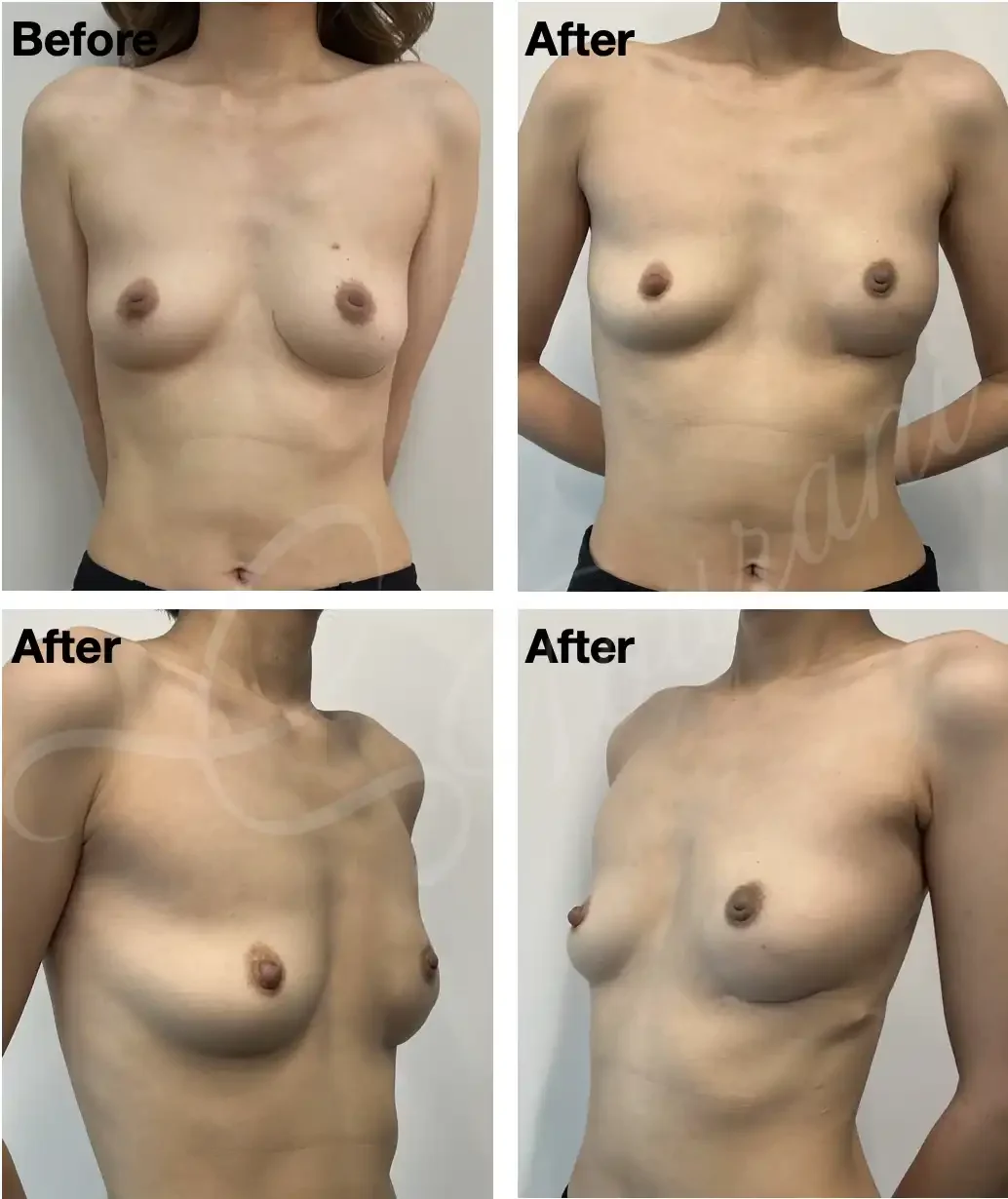
Case #305: 2 weeks post left nipple sparing mastectomy + immediate 1-stage implant reconstruction.
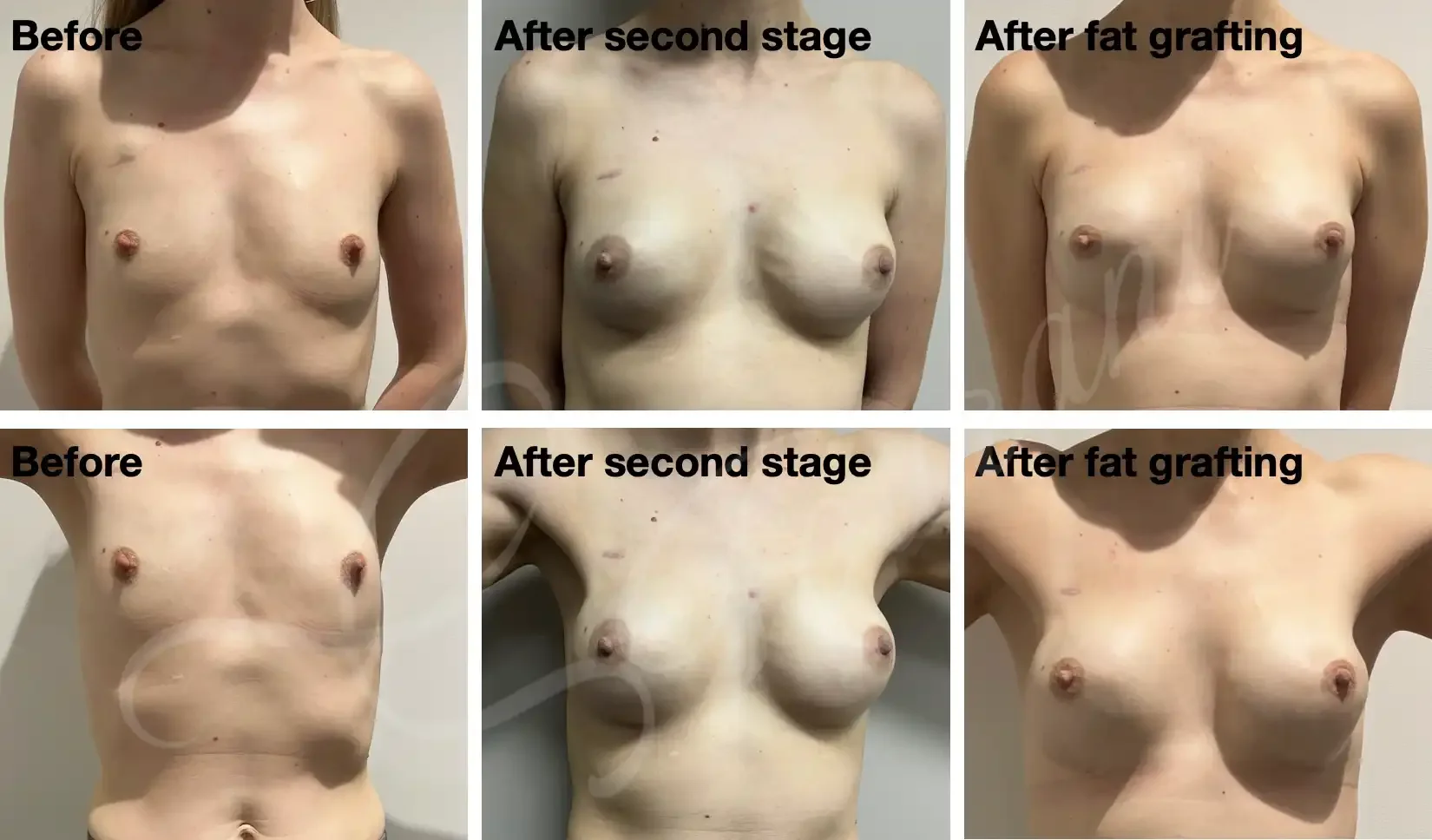
Case #306: Bilateral nipple sparing mastectomy + implant reconstruction (2-stage left, 1-stage right) for a triple negative left breast cancer. Final images 1 year post left breast lipomodelling to correct rippling.

Case #307: One year post right nipple sparing mastectomy + immediate 1-stage implant reconstruction.
Case #308: 1 year post skin sparing mastectomy + immediate 2-stage implant reconstruction.
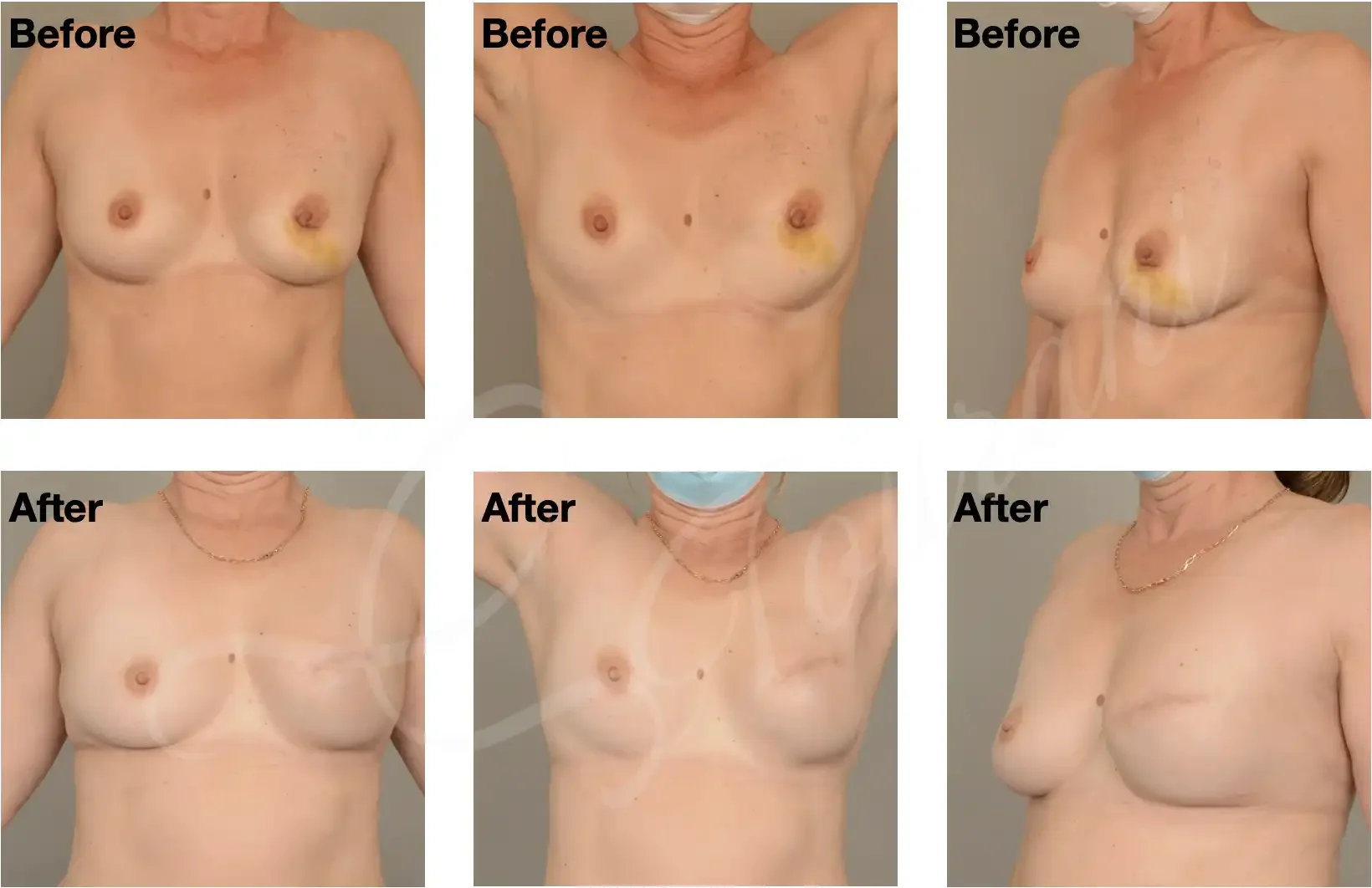
Case #309: Left nipple sparing mastectomy + immediate 1-stage implant reconstruction. Images are 1 year following radiotherapy.
Case #310: Right nipple sparing mastectomy + immediate 1-stage implant reconstruction. Images are flowing radiotherapy.
Case #311: One year following left skin sparing mastectomy + immediate 2-stage implant reconstruction.
Disclaimer: The images displayed are of actual patients of Dr. Saam Tourani who have provided informed consent. Please note that surgical results are individual and will vary based on patient anatomy, health, and healing processes. These photos are for educational purposes only and do not constitute a guarantee of a specific outcome.
Frequently Asked Questions
-
Breast reconstruction surgery refers to procedures used to restore the shape and appearance of the breast following mastectomy or major breast surgery. Reconstruction may involve implants, your own tissue (autologous reconstruction), or a combination of techniques depending on your anatomy, cancer treatment plan, and personal goals.
-
Yes. Immediate breast reconstruction is performed during the same operation as mastectomy and is commonly offered to suitable patients. In some situations, delayed reconstruction may be recommended after completion of cancer treatment such as radiotherapy or chemotherapy.
-
Breast reconstruction broadly falls into two categories:
Implant-based reconstruction
Autologous (tissue-based) reconstruction using tissue from another part of the body, such as a DIEP flap
Some patients may also benefit from hybrid techniques combining implants and autologous tissue.
-
A DIEP (Deep Inferior Epigastric Perforator) flap reconstruction uses excess skin and fat from the lower abdomen to recreate the breast without sacrificing the abdominal muscles. It is considered one of the most advanced forms of autologous breast reconstruction and can provide a natural look and feel.
-
Breast reconstruction is generally considered safe when performed by experienced surgeons. As with any major surgery, there are risks including bleeding, infection, wound healing problems, implant-related complications, and flap failure in tissue-based reconstruction. Your surgeon will discuss these risks in detail during consultation.
-
Breast reconstruction is carefully planned around your cancer treatment. In some cases, treatments such as radiotherapy may influence the timing or type of reconstruction recommended. Dr Saam Tourani works closely with your multidisciplinary breast cancer team to coordinate safe and personalised treatment planning.
-
Modern reconstructive techniques can achieve highly natural-looking results. However, reconstructed breasts may not have the same sensation as natural breast tissue, particularly after mastectomy. The final appearance depends on factors such as body shape, surgical technique, radiotherapy, and healing.
-
Recovery varies depending on the type of reconstruction performed. Implant-based reconstruction generally involves a shorter recovery compared with autologous tissue reconstruction such as DIEP flap surgery. Most patients require several weeks before returning to normal activities.
-
Yes. Nipple reconstruction and areola tattooing can often be performed as a later stage procedure once the reconstructed breast has healed and settled. Some patients may also be candidates for nipple-sparing mastectomy.
-
Some patients achieve their desired outcome in a single stage, while others may require revision procedures, fat grafting, implant exchange, symmetry surgery, or nipple reconstruction to optimise the final result.
-
Yes. Delayed breast reconstruction can be performed months or even years after mastectomy. Many women choose delayed reconstruction after completing cancer treatment or when they feel physically and emotionally ready.
-
In Australia, breast reconstruction following mastectomy is generally covered at least in part by Medicare and private health insurance, although out-of-pocket costs may still apply depending on the procedure, hospital, and level of cover.
-
Suitability depends on multiple factors including cancer stage, overall health, smoking status, body habitus, previous radiotherapy, and personal preferences. A detailed consultation is required to determine the most appropriate reconstructive approach.
-
Yes. Breast reconstruction often aims not only to restore breast volume but also to improve symmetry and body proportions. In some cases, surgery on the opposite breast, such as a lift or reduction, may be recommended to optimise symmetry.
Additional Resources
Breast reconstruction: https://www.bcna.org.au/resources/surgery-and-breast-reconstruction/breast-reconstructionBreast reconstruction: https://plasticsurgery.org.au/procedures/surgical-procedures/breast-reconstruction/
Breast reconstruction: https://www.bapras.org.uk/public/patient-information/surgery-guides/breast-reconstruction
Breast reconstruction decision aid: https://breconda.bcna.org.au/
Learn more about implant and tissue breast reconstruction with Melbourne specialist breast surgeon Dr Saam Tourani.